Angle Closure/ Narrow Angle Glaucoma
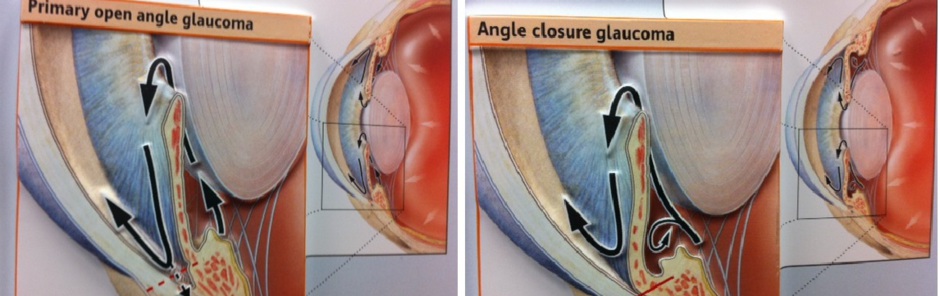
The 'angle' described here is the space/angulation between the cornea (the clear window of your eye) and the iris (the coloured part of your eye). It is at this angle that the 'trabecular meshwork' is situated which is responsible for drainage of fluid from the eye. In most eyes this 'angle' is wide open; however, it may be narrow or closed in some eyes. This narrowness might be responsible for raised eye pressure and may be responsible for a type of glaucoma called 'Primary angle closure Glaucoma' as opposed to 'Open Angle Glaucoma' where the drainage agle is open.
In a sub-set of such eyes when the 'angle' is totally/almost totally closed the eye pressure might be elevated to a dangerously high level (for example up to 60-70 mm Mercury as opposed the normal eye pressure range of 10-21 mm Mercury). This acute eye pressure rise is defined as 'acute angle closure' and is usually associated with eye pain, headache, nausea/vomiting, a history of intermittent blurring of vision with halos, red and watery eye, blurry vision, mid-dilated and non reactive pupil, and shallower anterior chamber of the eye. This condition is an eye emergency and urgent eye A&E referral is advised as otherwise the eye may sustain irreversible damage and reduction in vision. Please contact your local eye casualty / eye A& E for urgent appointment.
You will most likely require multiple medications including an injection to reduce your eye pressure quicky. Once your eye is comfortable, eye pressure is well controlled and your cornea (the front window of your eye) is clear you will most likely require Yag laser peripheral iridotomy ( creating a small holes in the coloured part of your eyes (iris), usually at about 12 o' clock meridian or under your upper eye lid. You will most likely require this for both your eyes.
You may also be advised UBM (Ultrasound Biomicroscopy) from Birmingham & Midland Eye Hospital to help long term management of your eyes. This particular investigation (UBM) might indicate that your natural lenses in the eyes are disproportionately large in comparison to the size of your eye. In such a circumstance a lens removal and insertion of an artificial intraocular lens to replace the natural lens may be advisable (this is exactly the same as a cataract surgery the only exception being that your vision may still be good and you may not necessarily have cataract). This surgery is primarily aimed at decongesting your eye, to create more space, to reduce eye pressure, to reduce your risk of glaucoma and risk of future acute angle closure. You will most likely require surgery in both your eyes for all the above mentioned reasons as well as to balance the (refractive) power of both your eyes.
Private & NHS patients
How to see Mr Raj
For private patients & referrals
Mr Akash Raj
Consultant Ophthalmologist, Glaucoma specialist & Cataract surgeon
Stourside Hospital (part of West midland Hospital)
60 Bradley Road
Stourbridge
DY8 1UX
01384 505 183
(Alternate:
Monday Evenings)
Appointments:
01384 912966
Private Secretary: Tara Ralph : 01384 632 636
Mr Akash Raj
Consultant Ophthalmologist, Glaucoma & Cataract specialist.
For NHS Referrals through GP/Opticians
Mr Akash Raj
Consultant Ophthalmologist (Glaucoma Lead)
Pensnett Road
Dudley
West Midlands
DY1 2HQ
Phone: 01384456111
Extn. 5815 (NHS Secretary: Lyn Eaton)